
15 Minutes to a Lifetime: How America Built a $19 Billion ADHD Amphetamine Retention Machine
A 15-minute checklist. No objective test. Schedule II stimulants. Four decades of dependency. The UK, Germany, France looked at these Meds and said no. America looked at it and said: $19 Billion/Yr

Rxan Smith: Uncomfortable · Homepage | RxanSmithMedia.com | Debt Clock
Series / ADHD Medication
Rxan Smith

America put millions of kids on Schedule II amphetamines, reassured parents despite limited long-term data, collected five decades of patients who now can’t function without the pills, and called it medicine. The drug companies called it a growth market. Congress called it Thursday.
This Substack is reader-supported. To receive new posts and support my work, consider becoming a free or paid subscriber.
.buymeacoffee.com/rxansmith · paypal.me/phireballsports
Name a legal product that requires a federal DEA license to prescribe, cannot be phoned into a pharmacy, and usually must be picked up in person with government ID. It carries a Black Box warning for potential abuse. Yet, it is routinely prescribed to children as young as six after a fifteen-minute office visit. This industry generates nineteen billion dollars annually. It sits in the same DEA schedule as cocaine and morphine.
Welcome to the ADHD medication system. Make yourself comfortable. A lot of people can’t anymore without it.
◆ ◆ ◆
Part I: What We’re Actually Talking About
The Chemistry of Compliance
Let’s establish the pharmacology, because this is where the conversation usually dies before it starts. Adderall is amphetamine salts. Ritalin is methylphenidate. Different compounds, similar outcome: increased dopamine and norepinephrine activity, improving focus and task execution in the short term. These drugs are effective; that isn’t the debate. The question is what happens after decades of continuous use—and that’s where the evidence gets thinner than the confidence. When you modulate brain chemistry daily for thirty years, you aren’t just “fixing” a problem; you are managing an ongoing biological adaptation.
The pharmaceutical industry spent considerable energy framing these facts as “glasses for the brain.” This analogy is so pervasive, so casually deployed in doctors’ offices and school counselors’ meetings, that most people have stopped asking the obvious follow-up: what is your evidence for that, and does it hold up after forty years of continuous use?
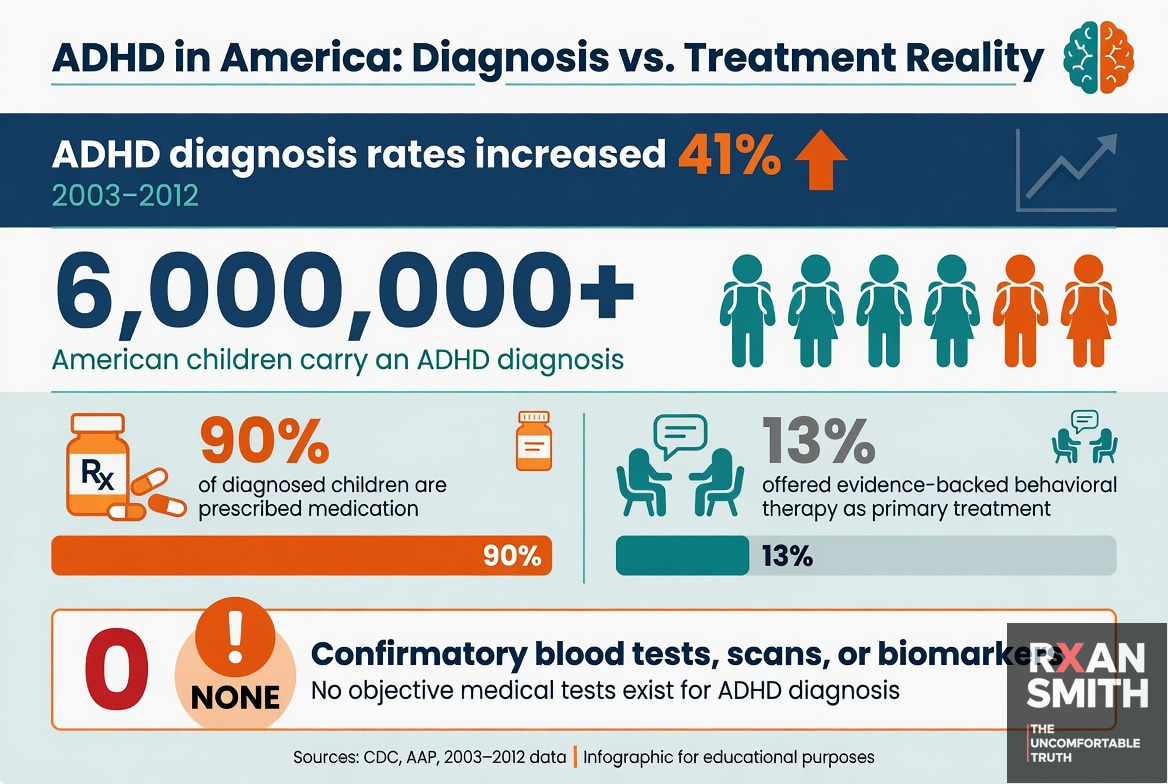
There is no blood test, no brain scan, no biomarker of any kind that can objectively confirm an ADHD diagnosis. The condition is real. The diagnostic tool is a symptom checklist evaluated in a fifteen-minute pediatrician appointment 90 percent of the time.— The Uncomfortable Position.
buymeacoffee.com/rxansmith · paypal.me/phireballsports
. Part II: The Diagnosis Problem
A Disease That Fails Its Own Audit
Try to name another condition for which American medicine routinely prescribes a federally controlled stimulant for decades without a single objective confirmatory test. You cannot, because there isn’t one. Diabetes gets blood panels. Cancer gets biopsies. Heart disease gets imaging. ADHD gets a checklist and a clock, and if the pediatrician is running behind, that clock runs fifteen minutes.
The literature has documented this gap explicitly. Researchers publishing on ADHD diagnosis in peer-reviewed psychiatry journals have concluded that the condition relies on “subjective reports” of symptoms that are “seldom, if ever, observed directly, let alone measured, by the diagnosing physician.” The diagnosis lives entirely in the DSM-5, defined not by neurological evidence but by a behavioral threshold that has expanded multiple times in forty years. The CDC documented a 41 percent increase in child and adolescent diagnoses between 2003 and 2012 alone. A systematic review of more than 334 published studies, appearing in a leading peer-reviewed medical journal, concluded that ADHD is overdiagnosed in children and adolescents, and that for kids with milder symptoms, the harms of diagnosis may frequently exceed the benefits.
A 15-minute checklist to start a 40-year pharmaceutical relationship is not medicine.
It’s a sales funnel in a stethoscope.
The relative age effect is the most damning illustration of how the diagnostic process works in practice. Children born in the final months of the calendar year, who are developmentally younger than their classmates simply because of when their birthday falls, are diagnosed and medicated at significantly higher rates. A child whose classmates are ten months older will look less focused, less organized, less capable of sitting still. A teacher fills out a checklist. A parent takes that checklist to a doctor. The doctor, working from exactly the same subjective symptom criteria, prescribes a federally controlled substance. Nobody pauses to ask whether the child is medically disordered or just younger..
Part III: What Gets Skipped
The Therapy Gap Nobody Wants to Talk About
The United Kingdom does not treat ADHD the way the United States treats ADHD. British clinical guidelines recommend medication as a first-line treatment only for children with severe symptoms. For moderate cases, behavioral therapy comes first, and medication is considered if therapy fails or is refused. This is not because Britain is philosophically opposed to pharmacology. It is because behavioral therapy for ADHD, including parent training, classroom supports, and occupational therapy interventions, has a substantial evidence base, and a child who develops coping strategies through therapy has something durable. A child who learns to function only with amphetamines has a dependency relationship that the prescribing system will need to maintain indefinitely.
In the United States, more than 90 percent of diagnosed children receive medication. Fewer than 13 percent receive the kind of evidence-backed behavioral therapy that research supports as effective. The doctors prescribing the medication follow up systematically, according to tracking data, at most 10 percent of the time. So the model is: diagnose quickly, medicate immediately, and monitor rarely. In any other medical context, this would be considered negligence. In the ADHD industrial complex, it is considered throughput.
Why does therapy get skipped? Because insurance doesn’t reimburse it the same way. Because a thirty-minute therapy session requires trained specialists who are in short supply. Because a prescription takes four minutes and a pharmacy handles the rest. Because the economic incentives of American healthcare reliably favor the billable procedure over the durable outcome. The drug companies understood this before most doctors did, and they built their market strategies around it. This isn’t unique to ADHD. It’s part of a broader structural failure in how America funds care over outcomes — one that shows up in nearly every corner of the system
Healthcare Cost Control (Ep. 2)
Why the system favors the billable procedure over the durable outcom
American Healthcare: The Billing System with a Waiting Room

MAKE AMERICA GROW AGAIN · Episode 2 of 25 · Root Fix · Full Series Index
Thanks for reading! This post is public so feel free to share it.
This Substack is reader-supported. To receive new posts and support my work, consider becoming a free or paid subscriber.
buymeacoffee.com/rxansmith · paypal.me/phireballsports
. ◆ ◆ ◆
Part III-B: One Story (That Belongs to Millions)
He Was Nine When the Teacher Flagged Him
He couldn’t sit still. Talked too much. Lost focus halfway through assignments. His parents did what responsible parents do: they listened, they scheduled the appointment, they trusted the system. Fifteen minutes later, he had a diagnosis and a prescription.
By high school, he was a different student. Focused. Productive. Efficient. The kind of outcome teachers point to as proof the system works. By college, he wasn’t taking the medication to fix a problem anymore. He was taking it to keep up. Then to get ahead. Then, without quite noticing the transition, to function at all. He tried to stop once, sophomore year. Slept fourteen hours a day. Couldn’t start a sentence, let alone finish a paper. He went back on it within a week.
He graduated with honors. Good job. Solid life on paper.
He still doesn’t know if he ever learned how to focus on his own. That’s not a complaint. That’s a question the system was never designed to answer, because the system is not structured around that question. It’s structured around the next refill.
He’s in his late thirties now. First prescription at nine. Then a slightly larger dose. Then extended release. Then something newer when tolerance came in quietly, like a rent increase. He doesn’t remember what focusing felt like before the medication. He’s not being dramatic. That memory is just gone, replaced by a before that is more concept than experience.
Last year, he tried to stop. Not because he wanted to. Because he wanted to know if he could.
By day three, he couldn’t get out of bed. By day five, he couldn’t follow a conversation. By day seven, he went back to the pharmacy, showed his ID, and picked up his prescription like a man filling a water bottle at a well he cannot leave.
His doctor told him that’s how untreated ADHD presents.
He doesn’t have a study to cite. He has a pattern he cannot ignore. Every time he stops, the system gets worse. Every time he goes back on, the system tells him that proves the diagnosis was right. There’s no version of this story where the drug is the question. Only the answer.
He doesn’t know if he has ADHD. He knows he has a prescription. In this system, no one who profits from the ambiguity is required to resolve it.
◆ ◆ ◆
Part IV: The Long-Term Question
The Patients Who’ve Been on This for Forty Years
Adderall hit the market in 1996. Ritalin has been prescribed for ADHD since the 1960s. The first generation of children who were medicated through childhood, adolescence, and into adulthood are now in their forties and fifties. Many of them report the same cluster of experiences: they cannot stop taking the medication without losing basic executive function. They cannot wake up without it. They describe what clinicians call cognitive and motivational blunting when they go off the drug. They are, in the functional and pharmacological sense of the word, dependent.
This is not a conspiracy theory. It is physiology. Amphetamines work by forcing the brain’s dopamine system to operate at an elevated state. The brain, which is adaptive by design, responds to sustained artificial stimulation through tolerance and neuroadaptation, meaning over time the same dose produces diminishing effects and the brain increasingly calibrates around the drug being present. Long-term stimulant use is documented to produce withdrawal effects, tolerance, and dependence. What remains unsettled in the scientific literature is not whether these adaptations occur, but how durable they are and at what point, if any, they become irreversible. That distinction is important. It is also the gap that the pharmaceutical industry has shown no commercial interest in closing.
A patient on Adderall for forty years is a patient generating forty years of prescription revenue. A patient who successfully transitions off medication through therapy is a former customer. The long-term safety literature is, as multiple review papers note, “not well known.” That is not an accident of science. It is an outcome the market selected for. When profit determines priority, outcomes become secondary — and that pattern isn’t limited to pharmaceuticals. (See: Make America Grow Again, Ep. 17 — Corporate Capture)
The pharmaceutical industry built a product that works well enough in the short term to generate referrals, creates enough dependency in the long term to ensure retention, and is covered by enough diagnostic ambiguity that the liability never quite lands where it belongs.— The Structural Argument
That is not an accident of science. It is an outcome the market selected for
Corporate Capture | Puppet Show of Democracy

Stop Scrolling: Our Democracy Was Sold While You Were Googling “How to Afford Insulin”

◆ ◆ ◆
Part V: Vyvanse, or How to Sell the Same Drug Twice
The Rebrand That Cost You Three Grand a Year
Vyvanse is lisdexamfetamine dimesylate, a prodrug that your body converts to dextroamphetamine after you swallow it. Dextroamphetamine is the active ingredient in Adderall. Vyvanse is, pharmacologically, a delivery mechanism for the same core stimulant that has existed since the 1930s. The distinction Shire, and later Takeda, marketed was the prodrug design: because the conversion step happens in the gut, the drug has a slower onset and is harder to abuse by snorting or injection. That is a genuine improvement. It is also, from a market strategy perspective, a patent extension vehicle.
Vyvanse launched in 2007. For the next sixteen years, it enjoyed full patent exclusivity. During that period, Takeda reported peak annual sales exceeding three billion dollars. The branded version cost over thirteen hundred dollars for a hundred-day supply. The molecule inside was dextroamphetamine. The patent on the molecule itself expired years earlier. What was protected, and what generated billions in revenue, was the specific delivery design and the strategic expansion of indications.
That expansion is worth examining. Vyvanse received FDA approval for binge eating disorder in adults in 2015. This was not incidental. By the time the ADHD patent was approaching its cliff, Takeda had a new patient population, a new indication, and a new argument for why the brand deserved continued premium pricing. Binge eating disorder is a real condition. Whether lisdexamfetamine is the best treatment for it, or whether it is the treatment Takeda could most profitably market for it given existing infrastructure and regulatory relationships, is a question the market does not particularly reward asking.
The patent expired in August 2023. Generics entered the market the same day. Branded Vyvanse sales dropped by a projected 60 to 75 percent in the first year. The architecture of the business, from the prodrug design to the indication expansion to the pediatric exclusivity extensions, was built precisely to delay that moment for as long as legally possible while extracting maximum revenue in the interim. That is not corruption. That is the system operating exactly as designed.
◆ ◆ ◆
Part VI: The Bureaucratic Maze
You Can’t Call It In, You Can’t Take It Across State Lines, and Good Luck
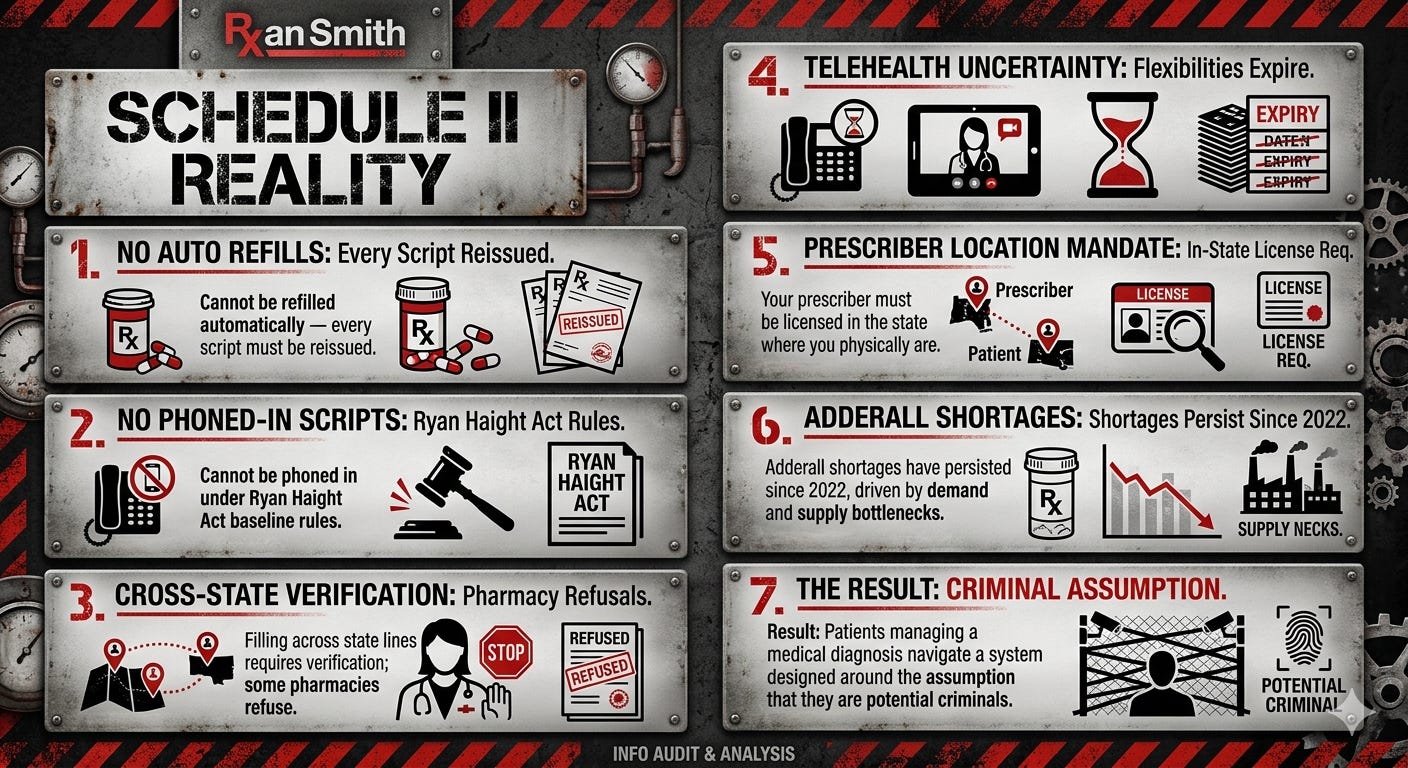
Here is the practical experience of being a legal Adderall or Ritalin patient in the United States. Your medication is a Schedule II controlled substance. It cannot be automatically refilled. Every prescription must be manually issued by your provider. In most states, under normal federal law, you cannot receive a new prescription via phone call. You must be seen, in person or via qualifying telehealth, every time. If you move to another state, or travel there, filling your existing prescription may require extra verification, and some pharmacies will refuse entirely. If you use a telehealth provider, that provider must be licensed in the state where you are physically located at the time of the visit.
The DEA has extended pandemic-era telehealth flexibilities, which loosened these rules temporarily, multiple times. As of this writing, those extensions run through 2026. After that, the Ryan Haight Act’s original requirements, including mandatory in-person visits before any Schedule II prescription, are expected to reassert themselves. The same federal classification system that places your ADHD medication in the same controlled substance schedule as cocaine and morphine will then require you to physically appear before a physician to legally treat the condition they’ve defined as a medical disorder. Which is, if you slow down and think about it, a remarkable thing to require of someone who has been continuously diagnosed and continuously prescribed for twenty consecutive years.
Meanwhile, the DEA has proposed rules for a special telehealth registration system that, in its most recently discussed form, would require prescribers to be physically located in the same state as their patients and issue at least half their prescriptions after in-person appointments. The telemedicine companies that built their businesses during the pandemic flexibilities faced federal scrutiny and in some cases criminal prosecution for prescribing practices. One platform’s CEO was convicted in 2025 for inappropriate stimulant distribution. The lesson the DEA appears to have drawn is that access was too easy. The lesson patients who lost their prescriptions when those platforms were shut down appear to have drawn is more complicated and rather more urgent
◆ ◆ ◆
Part VII: The Voice Problem
Who Gets to Complain About This
The people with the most evidence about what decades of ADHD medication actually does to the human brain are the people who’ve been on it for decades. They are also the least powerful voices in this conversation, for a specific structural reason: their dependence on the medication makes their experience easy to dismiss. A long-term patient who reports they cannot function without Adderall is told: that’s evidence the medication is working. A long-term patient who reports that stopping has caused persistent cognitive disruption is told: that’s evidence of untreated ADHD. The disorder explains the drug. The drug explains the disorder. The circle is closed, and the pharmaceutical company never has to appear in it.
A class action lawsuit representing four to five decades of adult patients who were first medicated as children, and who now report dependence, cognitive disruption, and inability to discontinue without significant impairment, would be among the largest in pharmaceutical history. The structural reason that lawsuit has not materialized is not complicated: proving causation across thirty years of individual medical history is difficult, the science remains genuinely contested in ways the industry’s lawyers can exploit indefinitely, and any physician willing to attribute a patient’s withdrawal symptoms to the drug rather than the disorder faces institutional pressure that has historically made that attribution professionally inconvenient.
The researcher who would study this doesn’t get funded to do so. The doctor who would say it out loud knows what happens next. And the patient who suspects it can’t prove it, because the experiment was never designed to be proven. It was designed to continue. A system that creates long-term dependency while calling it treatment starts to look like something that deserves its own conversation. (See: Make America Grow Again, Ep. 14 — Addiction Reform)A system that creates long-term dependency while calling it treatment deserves its own conversatio

There is no clean line between ADHD and Adderall for someone who has been on the drug since childhood. That ambiguity is not a failure of science. It is the most commercially durable asset the pharmaceutical industry has ever produced, and it was not an accident.
◆ ◆ ◆
The Bottom Line
What We’ve Actually Built Here
The American ADHD medication industry discovered that a disorder with no objective test, a diagnostic process that rewards speed, and a medication that creates long-term neurological dependency was, financially speaking, nearly perfect. Recession-proof. Retention-guaranteed.
The disorder is real. The medication helps many people. Both of those facts can coexist with the structural critique: when you find a medical condition that generates billions, creates a patient population that cannot easily discontinue treatment, and carries enough diagnostic ambiguity that liability never quite consolidates into accountability, you have found a business model wearing a white coat.
Stop calling it a mental health crisis when what you mean is a system that pathologized childhood behavior and responded with Schedule II medication. At some point, the dog ate so much homework that the dog became the homework.
I’m not here to tell you Adderall doesn’t work. It works. The argument is that a system which works well enough in the short term to generate referrals, but creates enough dependency in the long term to ensure retention, is a scandal. We don’t consider that a feature. Except in American healthcare, where we consider it a revenue stream.
A fifteen-minute checklist to start a forty-year pharmaceutical relationship is not medicine. It’s a sales funnel in a stethoscope. The UK looked at this system and declined. Germany looked at it and declined. America looked at it and said: nineteen billion dollars a year sounds about right.
See you next week for opiates. Bring your proof of ID.
— Rxan Smith · Rxan Smith: Uncomfortable · April 2026
Next episode: Opiates. Buckle up (more below).
The access exists. The effective care often doesn’t — a gap that runs through the entire system
Mental Health Access in America

You ever notice how we treat our minds like that junk drawer in the kitchen, full of tangled wires, old batteries, and receipts from 1999 that we swear we’ll sort out someday? Instead of cleaning it, we slam it shut and hope nothing spills out. That’s America’s mental health system: a carnival maze where you have to win the lottery just to talk to someone who won’t ghost you or deny your claim. It’s absurd that feeling human has become a luxury item locked behind red tape and fine print.
buymeacoffee.com/rxansmith · paypal.me/phireballsports
This Substack is reader-supported. To receive new posts and support my work, consider becoming a free or paid subscriber.
Thanks for reading! This post is public so feel free to share it.

Join Rxan Smith’s subscriber chat
Available in the Substack app and on web
Next episode: Opiates. Buckle up.
The Sackler family is in a museum somewhere with their name on the door. Shire is now Takeda. The kids who were put on Ritalin in 1987 are in their forties now, still filling prescriptions, still navigating shortage notices and state line restrictions and DEA extensions, still being told by a system built to retain them that the trouble they’re having is the disorder, not the treatment. The UK looked at this system and declined. Germany looked at it and declined. France looked at it and declined. America looked at it and said: nineteen billion dollars a year sounds about right.
See you next week for opiates. Same industry. Different product. Longer apology tour.
— Rxan Smith · Rxan Smith: Uncomfortable · April 2026
Big Pharma Miniseries · All Episodes
▶ Episode 1: Adderall, Ritalin, & Speed, Oh My: ADHD Meds (YOU’RE HERE)
○ Episode 2: The Pill That Ate America — Opiates [Coming Soon]
○ Episode 3: Calm Down or Stay Numb — Benzos & Antidepressants [Coming Soon]
○ Episode 4: Performance, Vanity, and the Weight of Profit — Sex, Hair & Weight Drugs [Coming Soon]
○ Episode 5: The Jab Economy — Vaccines & Elder Medications [Coming Soon]
○ Episode 6: The Whole Machine — Big Pharma & the Five Industries That Own “Healthcare” [Coming Soon]
Support Rxan Smith: Uncomfortable
$5 — You read it and it made you uncomfortable. Good.
$10 — You shared it because you knew someone needed to see it.
$25 — You’re the person in the room who actually says the thing.
$50 — You’ve been trying to explain this to people for years.
$100 — You want this work to keep existing, independently, for as long as it takes.
$250 — You understand that no sponsors means no compromises.
$500 — RXAN OWES ME.
buymeacoffee.com/rxansmith · paypal.me/phireballsports
I was diagnosed at 9 didn't really try meds till 32 was off them by 34